
How is Basal Cell Carcinoma (BCC) Treated?
The ultimate goal of treating basal cell carcinoma (BCC) is to completely remove the tumor with minimal impact on the surrounding area. Surgical techniques that remove BCCs are the most effective method of achieving cure. The most significant concerns with surgical treatment include tissue destruction and potential skin disfiguration that may result from removing the cancer along with healthy tissue on the edges of the cancer.
You will have a customized treatment plan depending on your tumor’s location and classification. Generally, BCCs have an extremely low rate of metastasis, less than 0.1%, and excellent prognosis. For example, the 5-year survival rate for most localized BCCs is close to 100%. Your healthcare provider will plan an appropriate treatment strategy after receiving the pathology report with details about your BCC. This will include the type of BCC, its size and location.
What are the Treatment Options for Basal Cell Carcinoma?
Below are descriptions of treatments approved and available for BCC. It is important to note that not all of the treatment options described will apply to every situation. Your healthcare provider will determine which treatments apply to your BCC.
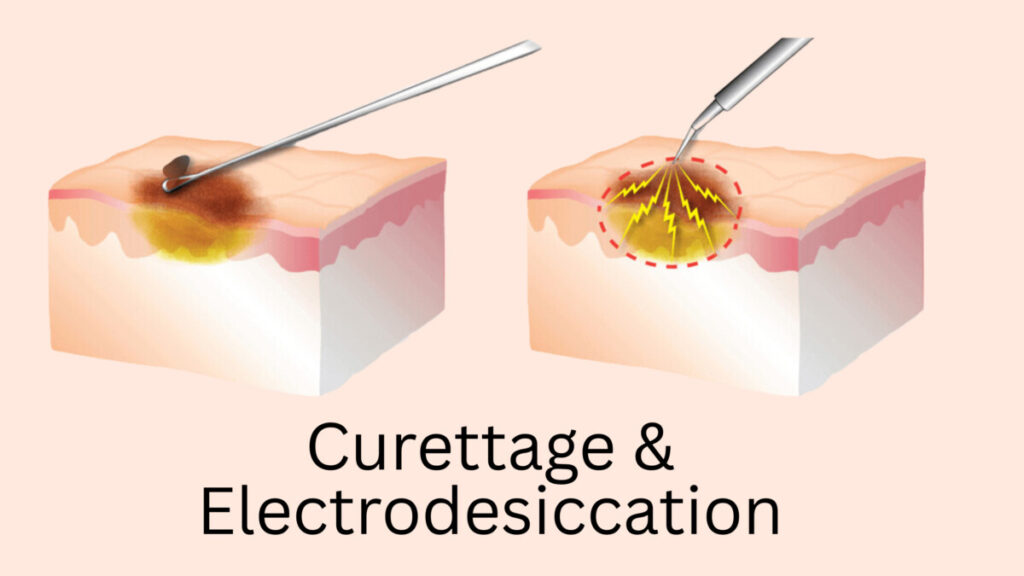
Curettage & Electrodesiccation
For curettage and electrodesiccation, the clinician scrapes the cancer from the skin with a sharp, looped tool called a curette, then immediately cauterizes the site. Electrodessication, the second step, prevents bleeding at the site without using sutures and burns off residual cancer cells. The wounded site will then be covered with gauze and heals with time. This procedure is a technique that is effective for superficial lesions like low-risk BCC. High-risk BCCs and areas with hair growth are unsuitable for this technique due to the potential for inadequate tumor removal and the risk of spreading.
Shave Excision
In this technique, the epidermal or dermal lesion is removed by sharp horizontal slicing of the skin. It is a quick procedure that can be performed in an office setting. The area is numbed with local anesthesia before removing the lesion with a scalpel or electrosurgical loop. The bleeding is immediately stopped with a special solution applied topically at the site prior to placing a bandage over the wound. Shave excision is recommended for low-risk BCCs detected on the trunk or other extremities. Layers of fat, subcutaneous tissue and deeper tissue are not removed in this technique. It is not suitable for pigmented tumors, cysts, or deep areas of concern. It may also leave a noticeable white scar.
After removing the tissue, the sample is sent to a laboratory for examination, where it will be assessed to make sure all the cancer has been removed along the margins of the tumor. On your pathology report, the terms negative, clean, not involved, or clear margins indicate that the tumor has been adequately removed, and is surrounded by normal tissue. If the areas around the tumor do not show healthy cells, you may need to have further excision during another appointment to obtain clear margins.

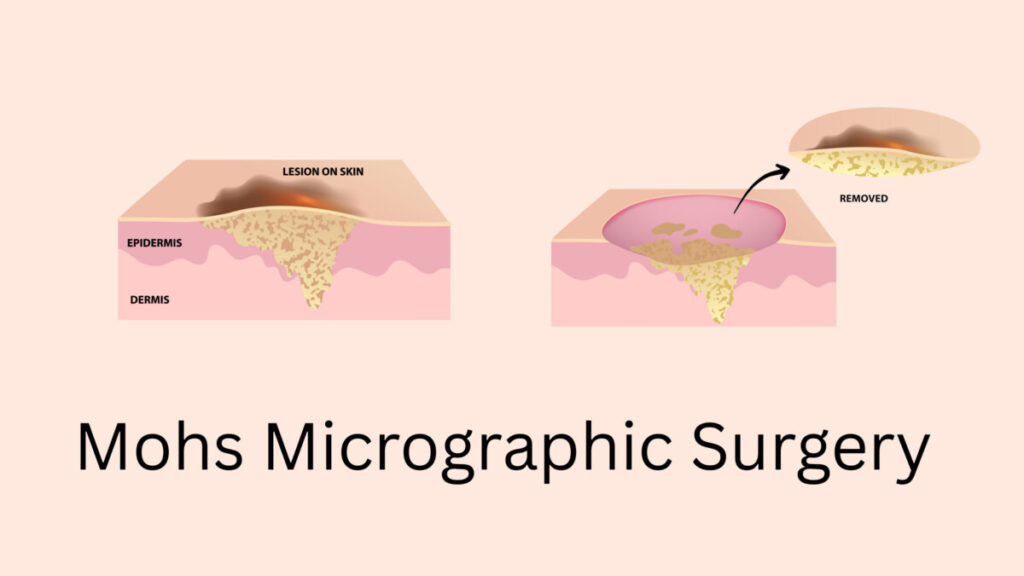
Mohs Micrographic Surgery
Mohs surgery is the preferred technique for removing high-risk BCC and re-excision of low-risk BCC. Studies have shown that after treatment, fewer people have recurrent BCCs if Mohs surgery was used relative to standard excision. Although it may be a superior technique, it requires a specialist certified in Mohs and is not appropriate for all cases.
Mohs surgery involves removing thin layers of skin one layer at a time and examining each layer under a microscope to determine if any cancer remains. Mohs incorporates a process by which the surgically removed tissue is carefully mapped, color-coded, and microscopically examined. Mapping allows the surgeon to pinpoint the location of the cells on the image back to the skin site. The mapped tissue edges and undersurface are then examined under a microscope to determine whether these areas contain normal or cancer cells. If cancer cells appear, the map specifies the region requiring additional tissue removal. Future excision will come from only that site, sparing healthy tissue that might otherwise be removed. Another layer is taken from the site with the cancer cells, and the process is repeated. Mohs surgery is complete once the tissue edges and undersurface are absent of cancer cells.
Radiation Therapy
Radiation involves concentrating a beam of energy on the tumor. The intense radiation will cause massive damage inside the cancer cells, which will lead to their death. This type of therapy is administered by a radiation specialist at a hospital or treatment center and may last six or more weeks.
Radiation therapy schedules vary among patients, and treatment could occur daily or two to four treatments per week, depending on each case.
Although surgical excision is usually the first treatment option, radiation therapy may be used for patients with low-risk, high-risk, or advanced BCC who are not eligible for surgery. It may also be used in patients as additional treatment after BCC excision if the cancer is high-risk or advanced, or if residual disease remains. It is not appropriate for individuals who inherited genetic conditions that predispose them to skin cancer because the radiation may cause cancer.

Cryotherapy
“Cryo” before the word “therapy” literally means icy cold therapy, a treatment which involves freeze and thaw cycles. This technique removes a BCC by spraying or holding it in contact with liquid nitrogen, a freezing liquid, for 30-60 seconds. The process may be repeated after a pause for thawing. Liquid nitrogen is -320 °F, which is sufficiently cold to damage normal human tissue. With this technique, it is used to freeze and kill the tumor. This rapid technique can be used instead of surgery to remove small BCCs. Patients with small, low-risk, or superficial BCCs may be eligible for cryotherapy.

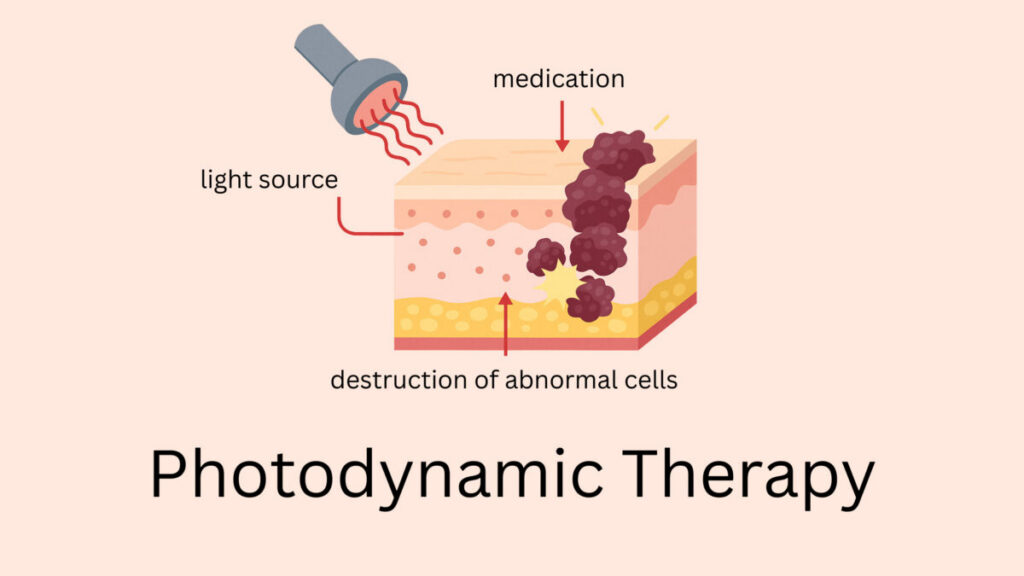
Photodynamic Therapy
Photodynamic therapy combines medicine with light to kill the tumor cells. In the first part of this technique, a medication that will later sensitize the cancer cells to light is prescribed. Examples of this medicine include 5-aminolevulinic acid and porfimer sodium. It takes a day or two for the cancer cells to absorb the light-sensitizing medicine. Then, a light with a specific wavelength of energy is focused at the BCC. This process creates toxic free oxygen radicals inside the cancer cells, which kills them. Superficial tumors (those that are small and/or not deep) may be ideal for this therapy. Light cannot completely penetrate deep or large tumors, which makes photodynamic therapy inappropriate for high-risk or advanced BCCs.
Topical Medications Applied to the Skin
In patients with low-risk BCC or superficial BCC or when a patient has numerous BCCs within a specific region, two medications can be used on the skin: 5-fluorouracil and imiquimod. These topical medications are also alternative options for patients who cannot have surgery or radiation therapy.
Topical 5-fluorouracil is a non-invasive and non-disfiguring method of killing the skin cancer cells. The topical solution is absorbed by the cancer cells, which mistake 5-fluorouracil for a metabolite they require to assemble DNA. The cancer cells cannot use 5-fluorouracil to make DNA, and will die due to missing this critical component. It also prevents the cell from manufacturing required DNA components.
Imiquimod is a drug that activates the immune system. For BCC it is prescribed as a topical cream. By generating an immune system reaction at skin sites where it is applied externally, imiquimod results in the death of cancer cells. Application may be several times per week for up to six weeks, depending on the case. Some applications of imiquimod may last longer. The skin may react with a rash, burning, or pain at the application site.

Medications for Advanced Basal Cell Carcinoma
Three medications are approved for specific cases of advanced BCC when locally advanced, nodal, and/or metastatic. Two medicines, vismodegib (Erivedge) and sonidegib (Odomzo), come in pill form and are targeted inhibitors of BCC growth. These drugs are sometimes referred to as hedgehog inhibitors. Another medication, cemiplimab (Libtayo), is administered through an intravenous infusion designed to activate the immune system.
Vismodegib (Erivedge) capsules are oral medications indicated for treating adults with metastatic BCC, or locally advanced BCC that has recurred following surgery, or adults who are not candidates for surgery and who are not candidates for radiation. This drug stops growth in BCC cells. It is taken daily at a recommended dose of 150 mg. The most common adverse reactions reported by people taking this medication are constipation, decreased appetite, diarrhea, distortion of taste, fatigue, hair loss, joint stiffness, muscle spasms, nausea, vomiting, and weight loss. Severe birth defects or embryonic death are a warning that accompanies this medication. Vismodegib cannot be used while pregnant or lactating, and all measures to prevent pregnancy must be strictly followed.
Sonidegib (Odomzo) capsules are oral medications indicated for treating adult patients with locally advanced BCC that has recurred following surgery or radiation therapy or those who are not candidates for surgery or radiation therapy. This drug is a targeted medication that stops growth in BCC cells. The recommended dosage is 200 mg once daily, taken on an empty stomach, at least one hour before or two hours after a meal. The most common adverse reactions reported by individuals taking this medication are abdominal pain, decreased appetite, decreased weight, diarrhea, distortion of taste, fatigue, hair loss, headaches, itching, muscle pain, muscle spasms, nausea, and vomiting. Severe birth defects or embryonic death are a warning that accompanies this medication. It cannot be used while pregnant or lactating, and all measures to prevent pregnancy must be strictly followed.
Cemiplimab (Libtayo) is an intravenous medication indicated for the treatment of patients with locally advanced BCC or metastatic BCC who have been previously treated with vismodegib or sonidegib, or patients for whom those drugs were not appropriate. Cemiplimab is a drug designed to generate an immune system reaction to the tumor cells. This drug is approved in other types of skin cancer and non-small cell lung cancer. For certain patients with advanced BCC, it may be the recommended treatment option. Cemiplimab is given in a clinic or hospital as an intravenous infusion over 30 minutes. It can be used every three weeks for up to two years. If this medication is taken alone, the most common adverse reactions include rash, itching, diarrhea, fatigue, muscle/joint pain, and/or gland dysfunction. Warnings that accompany this medication include the possibility of severe, potentially life-threatening inflammatory reactions, a reaction during the infusion, and embryo toxicity. Cemiplimab cannot be used while pregnant or lactating, and all measures to prevent pregnancy must be strictly followed.
Clinical Trials
Depending on the type of BCC you have, a clinical trial may open for enrollment and be appropriate to consider. Clinical trials are experimental research studies that test a new approach or therapy under the guidance of clinicians and a medical review board. These trials are entirely optional for patients. If current and approved treatments are not effectively treating your BCC, clinical trial options may be worthwhile to investigate.
